Indications
The primary use for abdominal free fluid assessment in the context of IM is for the detection of ascites as opposed to in the emergency medicine context where hemoperitoneum or perforated viscous are common queries but these should remain in the back our minds. In general this scan is useful for screening for decompensation with new ascites in known cirrhosis, undifferentiated abdominal distention, and procedural planning for paracentesis.
Acquisition/Interpretation
We use the same approach as the Focused Assessment with Sonography in Trauma (FAST) exam imaging the right upper quadrant (RUQ), left upper quadrant (LLQ), and pelvis in a systematic fashion. A positive scan is the presence of anechoic material that has irregular margins and settles into gravity dependent regions of the peritoneum in any of these views.
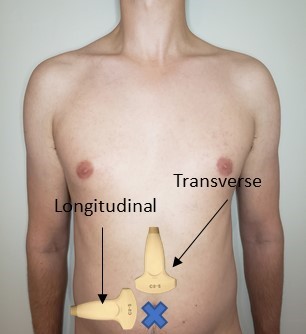
For this assessment we use the curvilinear probe.
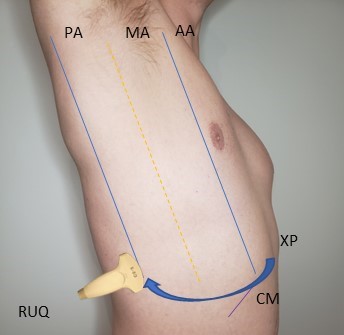
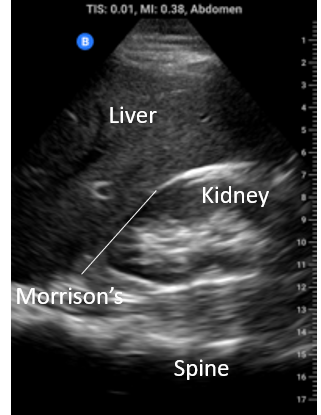
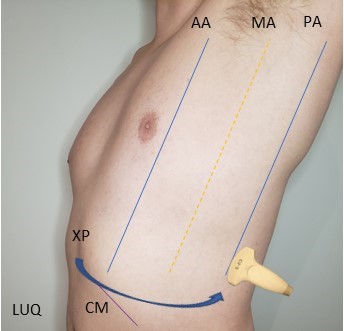
RUQ: Locate the xiphoid process and move laterally to the right mid axillary line or even the posterior axillary line over the ribs with the probe in the longitudinal orientation. Identify the liver and kidney and the interface between them, the hepatorenal interface or Morrison’s pouch. Fan anterior to posterior through the whole space looking for anechoic material. Be sure to interrogate the whole of Morrison’s pouch, the sub-diaphragmatic space and the caudal tip of the liver by fanning anterior to posterior through each of these structures. Fluid in any of these areas constitutes a positive scan.
LUQ: Locate the xiphoid process and move laterally to the posterior axillary line on the left side with the probe in longitudinal orientation and scan until both the spleen and left kidney are in the same view and focus on the splenorenal interface. This is only a landmark however as the splenorenal interface does not really allow for fluid accumulation. Instead slide caudally to sub-diaphragmatic space and fan anterior to posterior through the whole space. Anechoic material in this space is positive for free fluid.

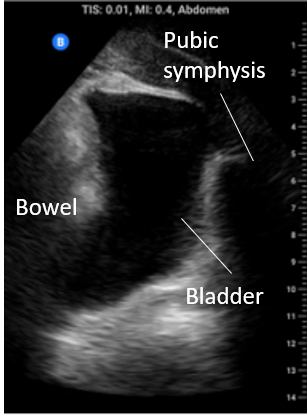
Pelvis: In the midline below the abdominal fold but superior to the pubic symphisis begin with the probe in transverse. Fan posterior to anterior through the bladder. In males pay particular attention to the rectovesical pouch and in females to the rectovaginal space (pouch of Douglas). Also look at the bladder edges for angular anechoic regions indicating fluid settling around the bladder and bowel.

Pearls
Caudal tip of the liver: The most sensitive point for detecting free fluid in the RUQ is the caudal tip of the liver.
Movement of free fluid: In the supine patient the pelvis is the most dependent part of the body and is the first place for free fluid to collect. However, the pelvis has a relatively small volume and quickly fills then moving to the right upper quadrant. The LUQ is the least dependent part of the abdomen. In cases free fluid originating in the LUQ, it flows following the splenocolic ligament preferentially to the RUQ.
LUQ: Unlike the RUQ where fluid accumulates preferentially in the hepatorenal interface, there is little potential space in the splenorenal interface. Therefore the more sensitive location is in the sub-diaphragmatic space in the LUQ.
Pitfalls
Intraluminal vs extraluminal free fluid: It is important to remember that there are numerous normal abdominal organs that are fluid filled e.g. blood vessels, stomach, gallbladder, and others that can become fluid filled in pathologic states such as small bowel or large bowel in the setting of obstruction. Especially if you are contemplating drainage you need to be certain you are draining abdominal free fluid. As a rule of thumb if fluid forms “corners” and sharp angles, settling into crevices, it is more likely EXTRAluminal and free flowing; see image on the left. If it has round borders it is most likely INTRAluminal or otherwise contained; see the image below on the right, that’s not ascites its a collection that was contiguous with bowel.

Complicated ascites: Though most of the abdominal free fluid encountered in IM is due to ascites from portal hypertension, exudative causes such as inflammatory, traumatic, and infectious collections that are non-gravity dependent or isolated to one part of the abdomen are also possible. Therefore it is important to not only look for abdominal fluid but also note its appearance as well. Notice in the images below the webbed and hazy appearance of the fluid; this patient had frankly purulent ascites requiring multiple abdominal drains.