Indications
One of the core applications of focused genitourinary ultrasound for the internist is to rule-in causes of obstructive acute kidney injury and obstructive nephrolithiasis through assessing for hydronephrosis.
Acquisition
For this assessment we use the curvilinear probe although the phased array on an abdominal preset is adequate. We scan three zones, right upper quadrant (RUQ) for the right kidney, left upper quadrant (LUQ) for the left, and bladder. The aim is to assess for dilated renal pelvis/calyces and/or a distended bladder.
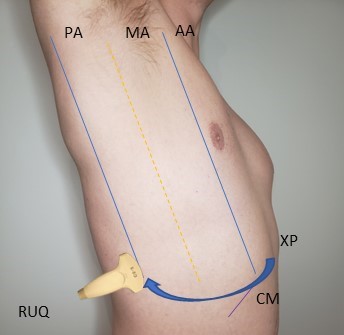
Right kidney: Locate the xiphoid process and move laterally to the right mid-axillary line or even the posterior axillary line over the ribs with the probe in the longitudinal orientation. Identify the kidney which is usually in the far field ‘below’ the caudal aspect of the liver and locate the calyces/renal pelvis which normally is hyperechoic surrounding by isoechoic/hypoechoic medulla/cortex. Fan through the kidney in both the longitudinal and transverse plane.
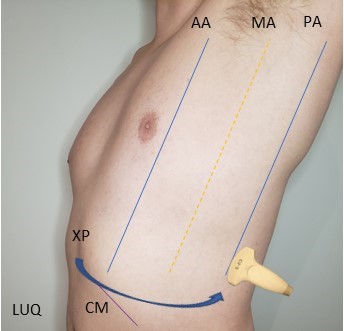
Left kidney: On the left side you will locate the xiphoid process and move laterally to the posterior axillary line on the left side with the probe in longitudinal orientation and scan until both the spleen and left kidney are in the same view and focus once again on the kidney calyces/renal pelvis. Fan through in the longitudinal and transverse planes.

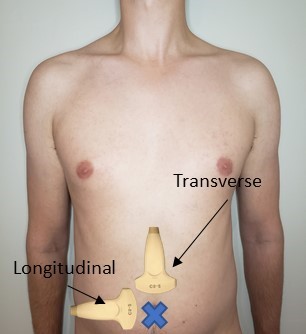
Bladder: The main intent of bladder scanning is to affirm in the setting of bilateral hydronephrosis whether there is a distended bladder or a collapsed bladder to establish whether hydro may be from the level of the bladder outlet or above. In the midline below the abdominal fold but superior to the pubic symphysis begin with the probe in transverse. Fan posterior to anterior through the bladder which when full should appear anechoic.

Interpretation
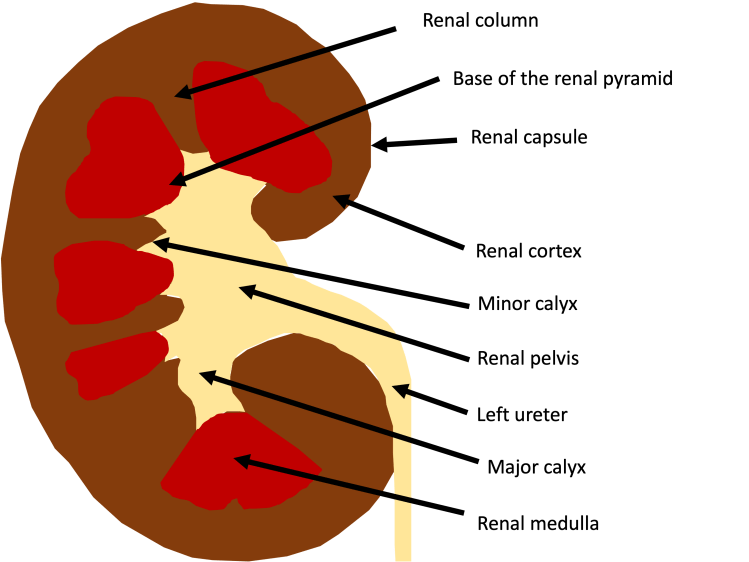
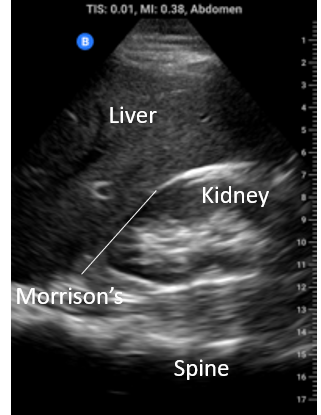
Normal Anatomy: For assessment of hydronephrosis it is particularly important to have a sense of the anatomy of the kidney in particular the collecting system from the minor to major calyces and on to the renal pelvis.
The normal renal collecting system should appear echo bright. The presence of anaechoic space is suggestive of hydronephrosis. Shown below on the left is a normal kidney while on the right is an example of moderate hydronpehrosis showing dilation of the renal pelvis and major calyces.

Though grading severity is more relevant to diagnostic imaging we consider it nevertheless important as it helps to frame the spectrum of pathology that can be seen as obstruction evolves. from an anechoic stripe within the renal pelvis to dilation of the major calcyces, minor calyces, and finally compression/thinning of the cortex.

Pearls/Pitfalls
Renal Cysts: One of the false positives of hydronephrosis are cysts arising from the cortex or the even more confusing medullary cysts. The key in either case is to look at the renal pelvis if its not anechoic there its not hydronephrosis. In the example on the left the patient has BOTH hydronephrosis and cortical cysts so you can see the difference side by side.

Prominent renal vessels: It is very common to be able to see the renal veins/arteries of the kidney . The is issue is the larger vessels traverse adjacent to the collecting system and can look quite convincing for hydronephrosis as the clip on the left shows. NB (yes there is free fluid as well)
This can be readily resolved by applying colour Doppler over the vessels (ensure the scale is set to 20 cm/s or below as these are not high velocity flows) and if flow is demonstrated it is not urinary stasis. In the images below the central anechoic stripe signalled by the green arrow on the left could be mistaken for low grade hydronephrosis but apply colour we see right away it is a vessel.

Contrast this with the image below where we can see there is no detectable flow in this anechoic space excluding prominent vasculature and ruling in hydronephrosis of moderate severity.
Extra-renal pelvis: In some normal individuals the renal pelvis exists OUTSIDE of the renal sinus which makes it much more distensible. Notice in this patient on the left the massive central “dilation” but without any calyceal dilation (left clip) which when viewed in transverse is seen to be outside of the renal sinus. This is precisely the reason which looking at the kidney in two planes is so important.
Bladder distension: If hydronephrosis is observed in the context of a full bladder this mandates an attempt at decompression especially in the context of bilateral hydronephrosis. If there is prompt resolution with catheter placement the cause can be diagnosed as related to bladder outlet obstruction.
